
Understanding and Overcoming Misophonia, 2nd edition (2017) is now available on Amazon.com and all major book sellers. Both printed and eBook formats.
Is Misophonia Ruining Your Life?
 The 2nd edition includes recent research of brain imaging studies and physical response studies of individuals when triggered. It includes over 50% new information compared to the first edition, including more management techniques, personal stories of individuals with misophonia and their families, treatment techniques for young children, and data on a treatment that reduces misophonia severity by 50%.Does the sound of other people chewing fill you with rage? Do certain sights and sounds make you crazy when they don’t bother anyone else? If so, you are not alone. Although not well known, misophonia is quite common, and there is hope. Are you tired of misophonia ruining your life? Are you ready to tackle your misophonia (or help a loved one)? If so, this book is for you.Recent brain imaging research indicates misophonia is a “soft-wired” neurological condition where a person has a strong emotional response of anger or disgust to specific sounds. The brain of a misophonic person being triggered does respond differently than someone without misophonia. The fMRI images are included.
The 2nd edition includes recent research of brain imaging studies and physical response studies of individuals when triggered. It includes over 50% new information compared to the first edition, including more management techniques, personal stories of individuals with misophonia and their families, treatment techniques for young children, and data on a treatment that reduces misophonia severity by 50%.Does the sound of other people chewing fill you with rage? Do certain sights and sounds make you crazy when they don’t bother anyone else? If so, you are not alone. Although not well known, misophonia is quite common, and there is hope. Are you tired of misophonia ruining your life? Are you ready to tackle your misophonia (or help a loved one)? If so, this book is for you.Recent brain imaging research indicates misophonia is a “soft-wired” neurological condition where a person has a strong emotional response of anger or disgust to specific sounds. The brain of a misophonic person being triggered does respond differently than someone without misophonia. The fMRI images are included.
Triggers for some might be hearing someone chewing. For others, it is the sound of sniffling or breathing. Many people also have visual triggers such as seeing someone chew gum. There are a lot of common triggers, but there are also some that are very unusual and unique. Almost any sound or sight can be a misophonia trigger for someone.
Misophonia can be upsetting and annoying, or it can be a debilitating condition. The book includes one story of getting Social Security disability for misophonia. Misophonia severity does vary, but it generally gets worse with time. There are important management techniques that are helpful to almost everyone.
Recent brain imaging research indicates misophonia is a “soft-wired” neurological condition where a person has a strong emotional response of anger or disgust to specific sounds. The brain of a misophonic person being triggered does respond differently than someone without misophonia. The fMRI images are included. The good news is that “soft-wired” brain connections can change.
Treatment for misophonia is still being developed and data collected. There are no published treatment studies on misophonia. Although there are no proven treatments that work for everyone, there are treatments that work for many. With proper management and treatment there is hope for reducing the horrible effects of this condition.
This book will help you understand what this mysterious condition is doing to you (or help you understand what someone close to you is experiencing). It explains how misophonia develops and expands with time, and why those little sounds cause a person SO much distress.
The book gives you many techniques that will help you manage this condition. Existing treatment options are described. There is hope.
With proper management and treatment, most people can greatly reduce the effects of misophonia in their life.
Developing misophonia has been a journey. Overcoming misophonia is also a journey, and it is a journey that can provide much relief for this horrible condition. It is journey that you should start today.
- Headings: A sample of Understanding and Overcoming Misophonia, 2nd edition (Chapters 1-6)
Table of Contents
1. The Misophonia Experience. 1
How to Determine if You Have Misophonia. 15
Proposed Diagnostic Criteria for Misophonia. 16
Rating the Severity of Misophonia. 16
Misophonia Activation Scale (MAS-1). 17
Amsterdam Misophonia Scale (A-MISO-S). 18
Misophonia Assessment Questionnaire. 22
Misophonia Questionnaire (MQ). 23
Misophonia Impact Survey (MIS). 26
Misophonia Emotional Responses. 34
The Individual Physical Reflex. 50
Involuntary Emotional Response. 55
Benefits of Understanding the Misophonic Physical Reflex. 63
Identifying Your Physical Reflex. 64
Environment and Misophonia. 75
Misophonia – An Aversive Conditioned Reflex. 79
Living with a Misophonic Husband. 91
Living with a Misophonic Wife. 92
Living with Misophonic Children. 93
Establish a Trigger-Free Haven. 97
General Health and Wellness. 98
Avoid and Escape Triggers. 101
Using Noise: Misophonia Management Protocol 102
Earplugs and Noise Cancelling Headphones. 110
Daily Muscle Relaxation Practice. 114
Overview of PMR and Applied Relaxation. 115
Muscle Relaxation as a Management Technique. 117
Guidelines for Progressive Muscle Relaxation. 118
Task Concentration – Selective Attention. 125
504 Plan Accommodations for Students. 129
Family Trigger Management Plans. 131
A Few Tricks with Technology. 132
Progressive Muscle Relaxation and Applied Relaxation. 135
Neural Repatterning Technique (NRT). 139
Misophonic Response and NRT. 140
Counterconditioning the Misophonia Reflex. 142
Hypnotherapy – Sequent Repatterning. 153
Sequent Repatterning Hypnotherapy plus NRT Success. 156
Psychosomatic Remediation Technique (PRT). 157
Medication for Anxiety or Depression. 164
Tinnitus Retraining Therapy. 164
Trigger Game: Pillow Fights, Wrestling, and Tickling for Children. 166
The Truth and Myth of Exposure Therapy. 170
Two Types of Kids Develop Misophonia. 174
Developing the First Misophonia Trigger. 175
Is Misophonia Caused by Genetics or Environment?. 176
- Misophonia or Conditioned Aversive Reflex Disorder (CARD) 181
- Misophonia Institute, a 501c3 Nonprofit. 183
Use your voice – speak up for yourself. 189
Neurofeedback Success Story. 190
Coping Well with Misophonia. 191
I Got Social Security Disability for Misophonia. 195
A Painful Life with Misophonia. 196
Downs and Ups of Misophonia. 199
Chapter 1. The Misophonia Experience
My Introduction to Misophonia
Friday, August 31, 2012. I was working as a parent coach when a mother contacted me asking for help with her difficult daughter and the disruption she was causing in their family. She explained the extreme behavior and her daughter’s unusual hatred of the breathing and eating sounds of her parents. She said it was called “misophonia” and there was no treatment for it. It was like a lightbulb went on in my head. All of a sudden, my daughter’s irrational complaining about my loud chewing made sense. My daughter had misophonia also. She was now an adult with her own children and one of them had misophonia also.
My retirement income supported me and I had extra time, so I decided to investigate misophonia. My training as a behavior scientist taught me that there were two general classes of human behavior. The first is purposeful behavior – the things we do. The second class of behavior is reflexes – all the things that our body does automatically, including emotions. Misophonia was clearly an emotional response, so I decided to apply my training to this new and mysterious condition. I love a challenge, and this was definitely a challenge. I love to help people, and this seemed like a worthwhile way to help my family and others.
I am also a very tenacious and determined person. When I set my mind to accomplish something, I stay focused and keep moving forward, despite surprises and roadblocks. Understanding misophonia has been an exciting challenge with many surprises and roadblocks. It has also been technically challenging developing methods to treat misophonia, including developing smartphone apps, but the opportunity to help others has been very rewarding. We have made great progress, but we still have much to do.
It is my hope that this book will help you understand misophonia. If you love someone with misophonia, I hope this book will give you an appreciation of what your loved one is experiencing. I also hope it will help you realize that misophonia is
a real condition and that the person can’t simply “snap out of it.” If you have misophonia, you are not crazy, and you were not just born this way. I hope this book will help you make immediate changes that can reduce the agony and emotional upheaval of misophonia, and that you will understand how you can start the process of overcoming this condition. It took years to develop all of your triggers, and it will take time to overcome them. I wish you well in your new journey to overcome your misophonia. So let’s get started.
Misophonia is a condition where a person has an extreme emotional response to commonly occurring soft sounds or visual images. These are called “triggers” because they trigger the emotional response of anger and disgust. The anger may be any form such as irritation, anger, hatred, or rage. Triggers also demand your attention, and when they are happening, they prevent you from thinking about anything else. If you’re reading this book because you think you have misophonia, you’re probably thinking, “How can little noises have such an overpowering negative effect on me? How (and why) do such noises cause me to feel such irrational anger or disgust, and a complete loss of control?”
If you’re reading the book because someone close to you has misophonia, you have probably thought it inconceivable that the misophonic person has such an extreme response to something as harmless as the sound of a crunch from eating a chip or a sniffle. This just doesn’t make sense. At least at some point, you probably thought, this is all in their head. This can’t be real. But it is real – very real. And it is likely more horrible than you can imagine.
In this book, I’ll present stories of real people with misophonia. Some are my clients, and others are those I have met along the way. Each gave their permission to have their story included because they want to help others understand this condition. I’ve changed their names for their privacy. Here are two typical stories from people just like you who hope to find relief from this debilitating condition.
Ryan’s Story
“I’ve dealt with misophonia since I was a child. I think it started around the age of six or seven. My parents would raise their voices when reprimanding me and I would quickly cover my ears and beg them to stop yelling at me. They weren’t even close to actually yelling at me, but on top of having this disorder, I also have above average hearing. I hear one pitch above and one pitch below the normal hearing range. This was medically proven by an ear, nose and throat doctor I went to, but because my mother talked through one of my hearing tests at the doctor, they thought I was half deaf.
“I find my triggers have continued to grow over the years. Chewing was really all that bothered me, but once I went to college my triggers grew at a staggering rate. I’m now triggered by any kind of chewing; even knowing someone is going to eat in the same room as me makes me get up and leave before they start eating because I have anxiety knowing what’s about to happen. Birds chirping (this started during my freshmen year of college because birds chirped nonstop outside of our dorm room window), pens clicking, nails tapping, the text message clicking sound, heavy breathing, noise through the wall of any kind, but especially the bass in music or people’s voices, sniffling, someone clearing their throat – the list goes on and on. Basically my misophonia has gotten to the point that any sound, if repetitive, will make me freak out. It’s like I’m constantly alert and my ears are always searching for trigger sounds, which is why I sleep with headphones and white noise and a box fan on high every night.
“My friends and family have known something was up for so long because the second I hear a trigger sound I turn and look at them with this ‘if you don’t stop making that noise I will kill you’ look, and they instantly stop what they’re doing and apologize. Their apology after they’ve stopped making a trigger sound makes me feel bad because they shouldn’t have to apologize for doing normal things like eating. Logically I know they shouldn’t have to alter their behavior because they’re not doing it on purpose and the sounds that bother me are normal everyday sounds, but in the moment all I can think about is that sound, and if I can’t remove myself – which I most often do – I will lose my mind and freak out. For example, I used to live at college and I could hear my neighbors through the wall of my room, and because I couldn’t get away from it I flipped and started banging on the wall and screaming at the top of my lungs, all while shaking with anger and rage flowing through my veins. Afterwards I felt stupid for flipping out, but I couldn’t help it, I couldn’t get away from the sound, and after about five minutes it feels like people are making sounds to purposely piss me off. Needless to say my dorm director called me a handful and I no longer live at college.
“Since finding misophoniainstitute.org (and misophoniatreatment.com) and showing the research to my family, they are much more understanding, my mother more than my father (his chewing is my biggest trigger in the entire world – even when he chews with his mouth closed – and he’s constantly biting his nails or his lip or the skin inside his mouth). By the way, Tourette syndrome runs in my family, and my sister and father have it, so you can imagine how difficult it is to have misophonia and live with people who can’t help but do things repetitively. Basically I’ve come to the point that I spend the majority of my time in my bedroom, alone. I don’t mind being alone, and frankly I feel less on edge when I’m by myself because I know that I’m not going to hear a trigger sound. On the other side of that coin is the fact that I live with my family, but I rarely see them because I’m constantly in my room. Additionally, sudden loud sounds make me jump out of my skin, so at this point being deaf seems like the only way I would be able to spend time around other people.
“I would love to learn any tips or anything that may help me and decrease my isolation. I love my family and I want to spend time with them, but I find it impossible to do so.”
Bill’s Story
“I feel like I know everyone else’s story by heart and can relate to all. After a recent crisis and diagnosis, I’ve been examining this (misophoniainstitute.org) and other sites like it. Thank-you to all who have shared their stories. I’ve struggled with the symptoms of this condition for as long as I can remember. The first vivid memory I have is during a 2,600-mile-long family road trip where I noticed my younger brother was breathing loudly. I alerted my mother, who assured me he was OK. In a short time this had escalated into yelling, and me positioning my head against the window and my bicep in such a way that I couldn’t hear him.
“This scene played out over and over in my family. Mealtimes were anxiety-provoking, and filled with anger, hurt feelings, abandonment, and self-loathing. I rarely ate with my folks and brother at mealtime. I rarely accompanied them on family outings. Believing I liked nature, I remember searching for secluded places outdoors. I wonder now if I wasn’t seeking some relief. University was hell – sniffles, gum chewing/popping, coughing, shuffling feet. Towards the end of my program I did not go to class but studied on my own or with a close friend. Miso has played a part in all my significant relationships, contributing to a divorce.
“I developed an addiction at an early age but have been sober for twenty-seven years (not always easy). It’s hard for me to overlook how the possibility of using a substance to manage miso could be problematic. I’m fifty-one years old now and feel like I’m starting something new again. As I said earlier, this diagnosis puts my life in a new perspective. I had forgotten about the mealtime anxieties and self-loathing, the look on my brother’s face when I’d look at him in rage and hatred. I hated myself for this; no one deserves those looks. I thought my mother hated me and regretted my birth. I can’t ignore how difficult life with me must have been. In the end I became a loner, finding it easier to be alone than with others. There have been significant people in my life, but miso has always surfaced.
“The aspect of this diagnosis that I find hopeful is how it may just be legitimate. I say that with respect to all that believe its legitimacy. I’ve spent my whole life being told and believing ‘it’s all in my head’ or ‘just ignore it,’ and believing that I was fundamentally broken. I’m in a relationship now with a reasonably understanding lady who says we can work this out. I hope we can, because I’m tired of believing I’m broken.
“I want to acknowledge how difficult it is for those around me and at the same time respect my struggles. I’ve never considered that maybe there is a possibility that this thing is beyond my control and that it is OK to ask for help. It sounds like a fairytale… thinking I can ask for help. I’ve got a lot of respect for all those who have put themselves on the line asking for help with this from those around them.
“Thanks for giving me this opportunity to express this.”
Misophonia Triggers
For a person who suffers with misophonia, his or her personal triggers are a central fact of life. A trigger is a sound or sight that causes a misophonic response. It may be a sound someone makes when chewing, a slight pop of the lips when speaking, or a person whistling. For a person with misophonia, a trigger causes an involuntary reaction of irritation, and if the trigger continues, the emotions quickly become extreme anger, rage, hatred, or disgust. These emotions are jerked out of the person, and trying to stay calm when being triggered is futile.
The immediate negative emotions to a trigger are the hallmark of misophonia. Along with the emotions come physiological (bodily) actions that go along with such emotions. These include increased general muscle tension, increased heart rate, sweating, and feelings of overwhelming distress. When the trigger ceases, the emotional upheaval generally continues. Many people continue to hear the sound in their mind and replay the experience in their mind. While it may only take a few minutes for a person to become extremely distraught from the triggers, it can take hours for the person to calm down and resume normal life.
The impact of misophonia can vary from almost nothing to debilitating. I met a man who has only one trigger, and it’s the sound of a spoon stirring a glass of iced tea. The tinkle sound is intolerable for him, but no one in his family drinks iced tea, so he rarely hears that trigger. His misophonia has little to no impact on his life. On the other hand, I met another person who also has only one trigger, and it is ruining her life. Her trigger is the sound of two or more women talking to each other. As a student in a mostly female discipline, she is subjected to this trigger continually at school, making her school experience hellacious.
Misdiagnoses
Many people with life-long misophonia have suffered because of being misdiagnosed. Traditionally, because virtually no one in the medical and psychological communities was aware of misophonia, any examination of an individual with misophonia resulted in a misdiagnosis. I asked members of an online misophonia support group to tell me their diagnoses prior to realizing they had misophonia. Here is a partial list: intermittent explosive disorder, oppositional defiant disorder, mood disorder, hyperacusis, ADD/ADHD, bipolar, paranoid personality disorder, obsessive compulsive disorder, anxiety, autism, nervous disorder, sensory processing disorder, phobia, typical mother-daughter issues, migraines, seizures, PTSD, and depression. Because any diagnosis without knowing about misophonia is a misdiagnosis, the best answer any professional could have provided was, “I don’t know.”
Additionally, many people have been told that there was nothing wrong with them. They were told they just needed to get on with their lives, or that they were spoiled brats, crazy, too sensitive, a prima donna, never happy, stuck up, or hypersensitive. Many were also told they needed to ignore the sounds or that it was all in their head. Misophonia causes extreme negative emotions and many individuals engage in inappropriate overt behavior (actions) directed against people they dearly love. Both the extreme emotions and actions cause high levels of guilt and shame, which is only made worse if the person is told it is their entire fault!
Here is a poem that expresses what it is like to have misophonia.
“My Misophonia”
By Angela Muriel Inez Mackay
My misophonia is not a quirk.
It’s not what “makes her different”
It’s not something fresh air can fix, or a pill can subside.
My misophonia is not intolerance.
It’s not an excuse to be “bitchy,”
and it is most certainly NOT that time of the month.
These tears are not from sadness.
They are from anger, and being overwhelmed.
They’re from the fear that it will be too much.
That it will push you away.
I do not wear headphones in defiance,
or in disrespect to your words.
I wear headphones for an ironic sense of quiet.
“It’s not you, it’s me” is my motto.
It’s what I repeat in my head while you chew,
Each bite slicing into my ears like knives,
Each scrape of the fork a flinch of my finger,
Each crumple of the bag a cringe.
It kills me when you take joy in my pain,
Your gum mocks me,
And instead of an apology, you say,
“It’s just a sound!”
To you, it IS just a sound.
But to me, it’s my worst nightmare.
To me,
It’s what makes me avoid people,
Avoid plans,
Avoid “grabbing a bite to eat” with friends.
It’s what makes me want to stay home,
It’s what makes me question why I even bother.
My misophonia is what fills me with fear
Every single day,
That I will be too much to handle,
That I’m too touchy,
That I’m too “intolerant”,
My misophonia is part of me,
And I’m sorry.
I’m sorry for every glare,
Every cringe,
Every snappy word.
I’m sorry,
I have misophonia.
“What is Misophonia?”
Written by Dr. Marsha Johnson, Audiologist, in her 20th year of providing clinical services to this population. Dr. Johnson is a co-founder of the Misophonia Association. (As discussed in the next chapter, Dr. Johnson was the first to identify misophonia as a distinct disorder.)
“Interviewers and researchers often ask, what is Misophonia?
“An official, medical association sanctioned definition is yet missing, but in the meantime, this is what I think.
“Misophonia is a thief, a monster, a silent and invisible hunter of the most vulnerable of our society – children. Misophonia picks its targets with intention, with sudden onset in many cases, before the victim has the cognitive or emotional capacity to recognize its intrusion – they suffer its effects. Misophonia is merciless, it attacks the most important human relationships we ever know, that between parent and child, between spouses, between brothers and sisters, between work colleagues. It forces its way into these close bonds and shreds them, snarls them, cuts them apart, and does not have a single regret.
“Misophonia is elusive, tricky, sophisticated and shifty. It cannot be seen with any diagnostic tool. It cannot be tracked into its hideous lair. It cannot be found in any particular tissue or bloodstream or organ. It spreads like a bad stink into every part of life and yet, cannot be grasped or photographed or measured. Misophonia can pass through generations, skipping at times, but spreading over time to the point where even non-affected family members or close friends, become infected to a certain degree with decreased sound tolerance.
“Misophonia is unreasonable, heartbreaking, vicious and driven. Despite heroic human hearts, full of resolve and fortitude, support and determination, it brings grown men to their knees, sends grown women hiding in back rooms, provokes children to defiantly scream their outrage and frustration, and drives family members to the end of their own ropes of tolerance and patience. Misophonia is unfair. It unceasingly picks at life and changes without reason. It asserts itself into occupational, school, and family settings. It will not play by the rules – there are no rules, and if there were, it would just cheat and change them all the time.
“Misophonia is everywhere, found in every culture, every people group, in every continent, every place where people live. It has been around for some time, unrecognized until the age of the internet and worldwide communication and sharing outed it from its deepest hiding spaces. Misophonia is unkind. It is unfair and unwilling to compromise. It is a bully – a seriously wicked condition that forces its chosen to feel unworthy, defective, unhappy, mentally ill, unreasonable, and sad. Too many times Misophonia forces its members to think and say, “Something is seriously wrong with me and I should be able to deal with this, and yet I cannot, so something is seriously wrong with me” (repeat). The most common words on the lips of those who have Misophonia who find out about it for the first time, as a name for their symptoms, their feelings, their reactions, their state of mind, their inability to cope with breathing, sniffing, chewing, clicking, speaking and other noises, is, “I Thought I Was Crazy,” then often, tears. As the thoughts now become, I am not crazy, this is real.
“Because Misophonia, whatever you are, wherever you are, you cannot have that. You cannot be that which makes one feel crazy, isolated, misunderstood, alone, apart or weird. We will not allow you to force these names onto these beloved and cherished human beings! And we are hunting you.
“We hunt you with as many weapons at hand as possible – sophisticated imaging machinery, genetic studies, psychological interviews and experiments, counseling and auditory applications. We hunt you and we will not stop until we drive you out of the thick jungle of tangles you hide in. Like all great scientific endeavors in the past, we will never give up. We walked on the moon and soon will be on Mars. You are nothing compared to the great acts that humankind has achieved, and we promise, we will hunt you down and tear away your camouflage until we see you, naked and tender, and so clear in our sights. And then we will simply destroy you. There is no alternative. Keeping in mind the streaming tears down young cheeks who suffer, on older cheeks who mourn, we hold this promise tightly. We are coming, Misophonia. We are strong, we are relentless, and we have created an army of hunters. You can count on it.”
2. Diagnosing Misophonia
Misophonia is an extreme emotional reaction to typically occurring sounds. “Miso” means dislike or hatred, “phonia” means sounds, so “misophonia” means ‘’a dislike or hatred of sounds.” This rather broad name was given to the disorder in 2001 by Drs. Pawel and Margaret Jastreboff.[i] I say “broad” because it’s not about hating sounds in general; it’s about hating only specific sounds. We call these trigger sounds. Additionally, the “hatred” of trigger sounds applies more to your involuntary response to a sound than your feelings about that sound.
This condition is also known as selective sound sensitivity syndrome, or 4S. This is the name given to this condition by audiologist Marsha Johnson, who first identified this condition in 1997.[ii] This is really a better name for the condition because there are specific and selective sounds to which the person is extremely sensitive. However, misophonia is the more popular name for this condition now, and it also includes visual triggers.[iii]
I have proposed that an even better name for this condition is Conditioned Aversive Reflex Disorder or CARD, which I will explain in a later chapter.
To define misophonia, let’s first describe what misophonia is not.
Misophonia is not a sensitivity to the volume of the sound or to how loud the sound is. That’s hyperacusis. Hyperacusis can either continue from childhood or develop in adulthood. It can be tested by an audiologist by measuring the volume at which sound becomes painful. There are specific treatments that have been shown to reduce hyperacusis.
It’s not a fear of a sound; that’s phonophobia. This is a condition in which fear is the dominant emotion. It includes the fear response from hearing a sound and the fear of being in a situation where a loud or specific sound may occur. This seems fairly common in children, such as when a child is scared by the toilet or the vacuum cleaner sound. A fear of sounds or a fear response to the sound is not misophonia, usually. I say “usually” because there are some individuals with misophonia that feel fear as part of their emotional response to triggers. Some feel fear as an immediate response to the trigger, and others experience a fear of more triggers occurring, similar to anxiety about possibly hearing more triggers. But misophonia will also include a strong anger or disgust response that accompanies the fear, and it will generally be in response to specific soft sounds which makes it distinct from phonophobia.
Sensory Processing Disorder (SPD) can cause an intolerance of loud sounds. SPD is a condition where a person has significant problems with multiple forms of sensory input such as touch, taste, smell, sight, and sounds. SPD is a general heightened sensitivity to sensory stimulation. It is not the same as misophonia, and it is not related to misophonia.[iv] A person with SPD may appear to have hyperacusis or phonophobia because of the way he or she reacts to sounds.
Misophonia is not being irritated or upset by a continuous, loud, intrusive, or an irritating sound. There are people who, when they are in a situation where there’s a repeating sound, become very upset. The sound can be soft but continuous, such as traffic noise heard inside their home. These people are generally considered a highly sensitive person (HSP). Their level of tolerance for these obnoxious or irritating situations is not as high as with most other people. And so they get upset. For example, a person living near an airport says that they have an extreme emotional reaction to the sound of airplanes flying over. This may or may not be misophonia. Misophonia is being upset (triggered) by a single occurrence of the trigger. Suppose they are not upset by the sound of a single airplane, but are upset by the first airplane in the morning, knowing that many more will follow. This is more likely to be a case of HSP than misophonia; they are upset because they know they will be hearing airplanes all day long. And the airplane noise is going to be intrusive and irritating. This person may be very, very, very distressed by the noise, and the extreme emotions may be identical to the emotions from misophonia. The level of distress does not determine whether a person does or does not have misophonia. The determining factor for misophonia is that a person triggers – has an immediate response of irritation or disgust – to a single instance of the trigger stimulus.
A person who is highly sensitive can also have misophonia. There may be certain sounds to which they are sensitive to because they are irritating sounds, but there are other sounds that are misophonic triggers.
Finally, misophonia is not reaction to a sound like fingernails on the chalkboard, a baby crying, a knife on a bottle, a disc grinder, or a female scream. It is common to be irritated by these sounds. They are some of the top ten most irritating sounds. It seems that we are genetically wired to respond to these sounds because they are similar in frequency to a baby crying – a sound which should make us take action.
With misophonia there is an immediate reaction to the trigger stimulus. The trigger stimulus generally takes the form of sounds or sights, and the stimulus causes an immediate and involuntary response. It’s a response that is jerked out of the person.
The triggers are generally soft sounds or common sights. If you don’t have misophonia or if it’s not a trigger sound you may not even hear the sound; but for a person with misophonia, when someone across the room makes a trigger sound, such as popping their gum, they are going to hear it and feel it. This is common with a misophonia trigger.
There are also strong emotions with misophonia, the most universal being hate, anger, rage, disgust, resentment, and being offended. People with misophonia want to get away from the sound or make it stop, and in many cases they are thinking of a verbal or a physical assault on the other person. Although it is extreme to think about physically hurting someone because of a sound they are making, rarely do people with misophonia act out on these impulses.
How to Determine if You Have Misophonia
Suppose a person is triggered by a baby crying. This could be misophonia, but maybe not. The way to tell is to perform two tests. The general principle is that we need to rule out that the person is responding to the volume of the trigger or to the meaning of the trigger – in this case, a baby in distress. Both of these can be tested using a recorded trigger. First, test to see if the person is triggered by a low volume cry. The crying needs to be a real trigger with the volume reduced by distance or by playing the recorded crying at lower volumes. If the person is triggered regardless of volume, it is probably misophonia. Next see if the person is upset by the meaning of the trigger by making it obvious that you are using a recording. Because it is a recording, there is no baby in distress who needs to be helped, and the person knows the baby is not in distress. If the person is triggered to a soft sound (low volume crying) where the meaning (baby in distress) is not a factor, then the person has misophonia.
A person has misophonia if they have at least one trigger that creates the extreme emotional response in one setting. Of course, a clinical definition of misophonia will take into account the impact of the triggers on a person’s life, but such a level has not been specified by the Diagnostic and Statistical Manual of Mental Disorders (DSM) which is used by psychologists and psychiatrists, or the International Statistical Classification of Diseases and Related Health Problems (ICD) which is used by health care providers.
Proposed Diagnostic Criteria for Misophonia
In 2013 by Arjun Schröder and associates at the University of Amsterdam proposed diagnostic criteria for misophonia which only considered auditory triggers.[v] Recent research supports revising those criteria to include other sensory modalities (sight, vibration, smell, etc.) along with the nature of the misophonic response. The directors of the Misophonia Institute (Michelle Lopez, Chris Pearson, and Thomas Dozier) proposed revised diagnostic criteria for misophonia.[vi] The criteria include the preceding information in a format suitable for professionals. If you would like to read it, it is included as Appendix A.
Rating the Severity of Misophonia
There are three surveys I use to rate the severity of misophonia. These are the Misophonia Activation Scale, the Amsterdam Misophonia Scale, and the Misophonia Assessment Questionnaire. The Misophonia Activation Scale was developed by Misophonia-UK.org and is the simplest of the three. There is a fourth scale, the Misophonia Questionnaire[vii], which I will include below, but I do not have experience with it. All of these surveys have instances where the triggers are referred to as “sounds” or “sound problem” or other words implying auditory triggers. In all cases, you should complete the survey considering all of your triggers, without concern whether they are auditory, visual, tactile, vibration, or any other type.
Misophonia Activation Scale (MAS-1)
Please select the level that best describes what you experience.
Level 0: Person with misophonia hears a known trigger sound but feels no discomfort.
Level 1: Person with misophonia is aware of the presence of a known trigger person but feels no, or minimal, anticipatory anxiety.
Level 2: Known trigger sound elicits minimal psychic discomfort, irritation or annoyance. No symptoms of panic or fight or flight response.
Level 3: Person with misophonia feels increasing levels of psychic discomfort but does not engage in any physical response. Sufferer may be hyper-vigilant to audio-visual stimuli.
Level 4: Person with misophonia engages in a minimal physical response – non-confrontational coping behaviors, such as asking the trigger person to stop making the noise, discreetly covering one ear, or by calmly moving away from the noise. No panic or flight or flight symptoms exhibited.
Level 5: Person with misophonia adopts more confrontational coping mechanisms, such as overtly covering their ears, mimicking the trigger person, engaging in other echolalia, or displaying overt irritation.
Level 6: Person with misophonia experiences substantial psychic discomfort. Symptoms of panic, and a fight or flight response, begin to engage.
Level 7: Person with misophonia experiences substantial psychic discomfort. Increasing use (louder, more frequent) of confrontational coping mechanisms. There may be unwanted sexual arousal. Sufferer may re-imagine the trigger sound and visual cues over and over again, sometimes for weeks, months or even years after the event.
Level 8: Person with misophonia experiences substantial psychic discomfort. Some violence ideation.
Level 9: Panic/rage reaction in full swing. Conscious decision not to use violence on trigger person. Actual flight from vicinity of noise and/or use of physical violence on an inanimate object. Panic, anger or severe irritation may be manifest in sufferer’s demeanor.
Level 10: Actual use of physical violence on a person or animal (e.g., a household pet). Violence may be inflicted on self (self-harming).
Unwanted sexual arousal can occur with an intense misophonic response, as listed at level seven, but only one of my clients has ever mentioned this. I had several clients who reported an unpleasant sexual response reflex occurring at all levels of misophonia severity. This is explained later, but for now, I suggest you do not consider sexual arousal as a primary factor in determining your misophonia severity. Virtually everyone with misophonia has wide variation in their response to triggers based on the situation, the trigger, and how long it continues. I suggest you rate yourself at the highest level you experience in a typical week.
Amsterdam Misophonia Scale (A-MISO-S)
The Amsterdam Misophonia Scale (A-MISO-S) is an adaptation of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) and was developed by researchers in Amsterdam.[viii] The severity of your misophonia is determined by the sum of the points from these questions.
AMSTERDAM MISOPHONIA SCALE: Rate the characteristics of each item during the prior week up until and including the time you fill out this survey. Scores should reflect the average (mean) occurrence of each item for the entire week.
Q1. How much of your time is occupied by misophonic triggers? How frequently do the (thoughts about the) misophonic triggers occur?
0: None
1: Mild – less than 1 hr/day, or occasional (thoughts about) triggers (no more than 5 times a day)
2: Moderate – 1 to 3 hrs/day, or frequent (thoughts about) triggers (no more than 8 times a day, most of the hours are unaffected).
3: Severe – greater than 3 hrs and up to 8 hrs/day or very frequent (thoughts about) triggers.
4: Extreme – greater than 8 hrs/day or near constant (thoughts about) triggers.
Q2. How much do these misophonic triggers interfere with your social, work or role functioning? (Is there anything that you don’t do because of them? If currently not working, determine how much performance would be affected if you were employed.)
0: None
1: Mild – slight interference with social or occupational/school activities, but overall performance not impaired.
2: Moderate – definite interference with social or occupational performance, but still manageable.
3: Severe – causes substantial impairment in social or occupational performance.
4: Extreme – incapacitating.
Q3. How much distress do the misophonic triggers cause you? (In most cases, distress is equated with irritation, anger, or disgust. Only rate the emotion that seems triggered by misophonic triggers, not generalized irritation or irritation associated with other conditions.)
0: None
1: Mild – occasional irritation/distress.
2: Moderate – disturbing irritation / anger / disgust, but still manageable.
3: Severe – very disturbing irritation/anger/disgust.
4: Extreme – near constant and disturbing anger/disgust.
Q4. How much effort do you make to resist the (thoughts about the) misophonic triggers? (How often do you try to disregard or turn your attention away from these triggers? Only rate effort made to resist, not success or failure in actually controlling the thought or sound.)
0: Makes an effort to always resist, or symptoms so minimal, doesn’t need to actively resist.
1: Tries to resist most of the time.
2: Makes some effort to resist.
3: Yields to all (thoughts about) misophonic triggers without attempting to control them, but does so with some reluctance.
4: Completely and willing yields to all obsessions.
Q5. How much control do you have over your thoughts about the misophonic triggers? How successful are you in stopping or diverting your thinking about the misophonic triggers? Can you dismiss them?
0: Complete control.
1: Much control – usually able to stop or divert thoughts about misophonic triggers.
2: Moderate control – sometimes able to stop or divert thoughts about misophonic triggers.
3: Little control – rarely successful in stopping or dismissing thoughts about misophonic triggers, can only divert attention with difficulty.
4: No control – experience thoughts as completely involuntary, rarely able to alter thinking about misophonic triggers.
Q6. Have you been avoiding doing anything, going any place, or being with anyone because of your misophonia? (How much do you avoid, for example, by using other loud sounds, such as music?)
0: No deliberate avoidance.
1: Mild, minimal avoidance. Less than an hrs/day or occasional avoidance.
2: Moderate, some avoidance. 1 to 3 hrs/day or frequent avoidance.
3: Severe, much avoidance. Greater than 3 up to 8 hrs/day. Very frequent avoidance.
4: Extreme very extensive avoidance. Greater than 8 hr/day. Doing almost everything you can to avoid triggering symptoms.
Finally:
What would be the worst thing that could happen to you if you were not able to avoid the misophonic triggers?
Describe:
_________________________________________________
The sum score of these questions determines the severity rating as follows:
– 0-4: Subclinical (meaning you do not need treatment)
– 5-9: Mild
– 10-14: Moderate
– 15-19: Severe
– 20-24: Extreme
Misophonia Assessment Questionnaire
Marsha Johnson developed a survey for use with her clients. It’s called the Misophonia Assessment Questionnaire. The survey consists of 21 questions that are scored from 0 to 3 points based on how often the item applies to you. The severity of your misophonia is determined by the sum of the points from these questions.
When the survey says “sound issues” think “misophonia issues” because misophonia includes your response to any type of sensory input – sound, visual, vibration, smell, etc.
| MISOPHONIA ASSESSMENT QUESTIONNAIRE | |
|
RATING SCALE: 0 = not at all, 1 = a little of the time, 2 = a good deal of the time, 3 = almost all the time |
Score |
| 1. My sound issues currently make me unhappy | |
| 2. My sound issues currently create problems for me. | |
| 3. My sound issues have recently made me feel angry. | |
| 4. I feel that no one understands my problems with certain sounds. | |
| 5. My sound issues do not seem to have a known cause. | |
| 6. My sound issues currently make me feel helpless. | |
| 7. My sound issues currently interfere with my social life. | |
| 8. My sound issues currently make me feel isolated. | |
| 9. My sound issues have recently created problems for me in groups. | |
| 10. My sound issues negatively affect my work/school life (currently or recently). | |
| 11. My sound issues currently make me feel frustrated. | |
| 12. My sound issues currently impact my entire life negatively. | |
| 13. My sound issues have recently made me feel guilty. | |
| 14. My sound issues are classified as “crazy.” | |
| 15. I feel that no one can help me with my sound issues. | |
| 16. My sound issues currently make me feel hopeless. | |
| 17. I feel that my sound issues will only get worse with time. | |
| 18. My sound issues currently impact my family relationships. | |
| 19. My sound issues have recently affected my ability to be with other people. | |
| 20. My sound issues have not been recognized as legitimate. | |
| 21. I am worried that my whole life will be affected by sound issues. | |
|
Sum Score |
Dr. Johnson divided the scale into thirds. The lower third (0-21) is mild. The middle third (22-42) is moderate, and the upper third (43-63) is severe.[ix] You can take this survey and rate your misophonia. It would seem to make more sense to divide the scale into five zones, like the A-MISO-S survey. With five zones, the ratings would be
– 0-11: Subclinical (meaning you do not need treatment)
– 12-24: Mild
– 25-37: Moderate
– 38-50: Severe
– 51-63: Extreme
Misophonia Questionnaire (MQ)
The Misophonia Questionnaire was developed for a study at the University of South Florida, and it was also used in a recent doctoral dissertation[x]. The study considered a score of 7 or higher on the misophonia severity scale (part 3, 1-15 rating) to be “clinically significant.” This means that misophonia created a serious problem in their life that warranted seeking treatment. Adding the score of all 20 questions provides an overall measure of misophonia severity.
Part 1. Misophonia Symptom Scale
Directions: Please rate how much the following statements describe you on a scale from 0 to 4.
0: Not at all True
1: Rarely True
2: Sometimes True
3: Often True
4: Always True
In comparison to other people, I am sensitive to the sound of:
- People eating (e.g. chewing, swallowing, lips smacking, slurping, etc.).
- Repetitive tapping (e.g. pen on table, foot on floor, etc.).
- Rustling (e.g. plastic, paper, etc.).
- People making nasal sounds (e.g. inhale, exhale, sniffing, etc.).
- People making throat sounds (e.g. throat-clearing, coughing, etc.).
- Certain consonants and/or vowels (e.g. “k” sounds, etc.).
- Environmental sounds (e.g. clock ticking, refrigerator humming, etc.).
- Other: ______________________________
Part2. Misophonia Emotions and Behaviors Scale
Directions: If any of the aforementioned statements were given a value of “1 – Rarely True” or higher, please continue onto the following section and rate how often the subsequent statements occur, 0 being “Never” and 4 being “Always.”
0: Never
1: Rarely
2: Sometimes
3: Often
4: Always
Once you are aware of the sound(s), because of the sound(s), how often do you:
- Leave the environment to a place where the sound(s) cannot be heard anymore?
- Actively avoid certain situations, places, things, and/or people in anticipation of the sound(s)?
- Cover your ears?
- Become anxious or distressed?
- Become sad or depressed?
- Become annoyed?
- Have violent thoughts?
- Become angry?
- Become physically aggressive?
- Become verbally aggressive?
- Other: ______________________________
Part 3. Misophonia Severity Scale
Directions: Please rate the severity of your sound sensitivity on the following scale from 1 (minimal) to 15 (very severe). Please consider the number of sounds that you are sensitive to, the degree of distress, and the impairment in your life due to your sound sensitivities.
____ If you do not have any sound sensitivities, please check here.
1-3: Minimal within range of normal or very mild sound sensitivities. I spend little time resisting or being affected by my sound sensitivities. Almost no or no interference in daily activity.
4-6: Mild sound sensitivities. Mild sound sensitivities that are noticeable to me and to an observer, cause mild interference in my life and which I may resist or be affected for a minimal period of time. Easily tolerated by others.
7-9: Moderate sound sensitivities. Sounds sensitivities that cause significant interference in my life and which I spend a great deal of conscious energy resisting or being affected by. Require some help from others to function in daily activity.
10-12: Severe sound sensitivities. Sound sensitivities that are crippling to me, interfering so that daily activity is “an active struggle.” I may spend full time resisting my sound sensitivities or being affected by them. Require much help from others to function.
13-15: Very severe sound sensitivities. Sound sensitivities that completely cripple me so that I require close supervision over eating, sleeping, and so forth. It is hard to function on a day-to-day basis because of this.
Misophonia Impact Survey (MIS)
- Rate how misophonia has interfered with family life in the past two weeks. (If you have avoided these activities because of misophonia, include that factor in your rating.)
None Mildly Moderately Severely Extremely N/A
0 1 2 3 4 5 6 7 8 9 10 N/A
- Rate how misophonia has interfered with intimate relationships in the past 2 weeks. (If you have avoided this because of misophonia, include that factor in your rating.)
None Mildly Moderately Severely Extremely N/A
0 1 2 3 4 5 6 7 8 9 10 N/A
- Rate how misophonia has interfered with your social life and leisure activities with others in the past 2 weeks. (If you avoid these activities because of misophonia include that factor in your rating.)
None Mildly Moderately Severely Extremely N/A
0 1 2 3 4 5 6 7 8 9 10 N/A
- Rate how misophonia has interfered with your work / school work, including unpaid volunteer work, training, or similar activities in the past 2 weeks. (If you avoid these activities because of misophonia include that factor in your rating.)
None Mildly Moderately Severely Extremely N/A
0 1 2 3 4 5 6 7 8 9 10 N/A
- Rate how misophonia has interfered with your individual activities and alone time in the past 2 weeks. (If you avoid certain activities because of misophonia include that factor in your rating.)
None Mildly Moderately Severely Extremely N/A
0 1 2 3 4 5 6 7 8 9 10 N/A
Add all the numbers on the Misophonia Impact Survey and that is your total misophonia impact score.
These assessments can be a valuable way to track the progress of your misophonia over time. Because change in misophonia symptoms is often slow (whether increasing or decreasing in severity) and treatment programs can take six months or more, it can be beneficial to fill out these forms regularly to track your progress when you are engaged in a treatment program.
3. Triggers, Triggers, and More Triggers
Misophonia triggers generally start with a familiar person and a familiar sound. It is something in the person’s life. I conducted a survey of individuals with misophonia in 2013 in which two-thirds said their worst trigger was an eating/chewing sound, and 10% were breathing sounds. The remaining 25% had a variety of “worst triggers” including bass through walls, a dog barking, coughing, clicking sounds, whistling, parents talking, sibilance (the sound produced when saying words such as sun or chip), and someone typing on a keyboard. This is by no means a complete list of triggers. In fact, it is virtually impossible to make a complete list because a trigger can be virtually any repeating sound or sight. Although much less common, triggers can also be touch, smell, and vibrations.
Triggers are sounds we hear in everyday life. Eating sounds and dinner table sounds are very common in our lives, and are the most common triggers for misophonia. The second most common triggers are breathing or nose sounds, such as nose whistles, heavy breathing, sighing, snoring, and anything associated with breathing. In a large survey I ran last year, 94% reported eating/chewing sound triggers, but really, any repeating sound can be a trigger. The list of known triggers is like the list of all repeating sounds in the world.
It’s not that these sounds become triggers because of the sound itself. They become triggers because the person hears the sound in a specific situation and they develop a misophonic response to that sound.
As mentioned, we find that triggers start with one sound or one person making a particular noise, and then the trigger spreads to similar sounds, other places, anyone making the already offensive sound, and sights associated with those sounds. So with time these triggers spread and spread. We will cover this in detail in the chapter on Developing New Triggers.
Misophonia can start with a visual trigger, but this is rare. In fact, I have only talked to one person whose misophonia started with a visual trigger – a friend picking at their cuticles. In a 2015 survey of 1,067 people, only nine had misophonia start with a visual trigger, such as foot wiggling, leg bouncing, hair twirling, and leg crossing. That is less than 1%. Generally misophonia starts with an auditory trigger, and then visual images that occur immediately before the trigger become visual triggers. For example, if I trigger to chewing, then seeing someone put food into their mouth could become a trigger. I could also develop a trigger to seeing someone bring food toward their mouth or to picking up a potato chip.
Images that occur with the trigger can also become trigger stimuli. For example, jaw movement associated with chewing is commonly reported as a visual trigger by someone who triggers to gum popping.
It is probably possible for visual triggers to develop to images that occur in the same general time of auditory triggers. For example, if a person is triggered by eating sounds, specific voice sounds may be noticed at mealtime, and because the person is being triggered by eating sounds, the voice sounds could become triggers. We also find that repetitive movements such as leg jiggling or hair twirling are common trigger stimuli, but it’s not clear why. I had a client suggest it was because it was a nervous behavior, but I don’t have any data on this.
The next table shows the common misophonic auditory triggers with the percentage of participants who had one or more triggers in that category. The data is from a survey I took in 2015 with over 1,000 participants. Participants were recruited from misophonia Facebook groups, Yahoo groups, and individuals subscribed to my misophonia newsletter. Most of these individuals have misophonia that is sufficiently severe to cause their participation in these groups.
Sound (Auditory) Triggers:
| Sounds of people eating – all forms of chewing, crunching, smacking, swallowing, talking with food in mouth, etc. | 94% |
| Sounds made at the table – fork on plate, fork scraping teeth, spoon on bowl, clinking of glasses, etc. | 63% |
| Sounds of people drinking – sipping, slurping, saying “ah” after a drink, swallowing, breathing after a drink, etc. | 78% |
| Other mouth sounds – sucking teeth, lip popping, kissing, flossing, brushing teeth, etc. | 76% |
| Sounds associated with eating – opening chip bags, water bottle crinkling, setting a cup down, etc. | 55% |
| Breathing sounds – sniffling, snorting, nasally breathing, regular breathing, snoring, nose whistle, yawing, coughing, throat clearing, hiccups, etc. | 82% |
| Home sounds of people – voices/TV/music/bass through walls, door slamming, nail clipping, foot shuffling, flip flops, heavy footsteps, walking of people upstairs, joint cracking, scratching, baby crying, bouncing ball, etc. | 65% |
| Work/school sounds – typing, mouse clicks, page flipping, pencil on paper, copier sound, pen clicking, pen tapping, tapping on desk, etc. | 54% |
| Vocal triggers – consonant sounds (S and P especially), vowel sounds (not common), lip pop when speaking, dry mouth voice, gravelly voice, whispering, specific words, muffled talking, several people talking at once, “uh”, etc. | 51% |
| Singing, humming, whistling | 48% |
| Animal sounds – dogs/cat grooming, dogs drinking, dogs barking, rooster crowing, birds chirping, crickets, frogs, animal scratching, dog whimpering, etc. | 33% |
| Electronic sounds – phone ringtones, key clicks, alert tones, beeps, etc. | 28% |
| Home sounds of equipment – refrigerator running, hair dryers, electric shavers, ticking clocks, pipes knocking, lawnmowers, toilet flushing, etc. | 24% |
| Other – Farm equipment, pumps, back-up beepers, traffic noise, beep of car locking, car door slamming | 16% |
Sight (Visual) Triggers – open mouth chewing, jaw movement (chewing), hand touching face, scrolling on smartphone, pointing, leg jiggling, hair twirling, putting food into mouth, drumming fingers, blinking eyes, picking at fingernails
Odor (Olfactory) Triggers – certain scents (rare)
Touch (Tactile) Triggers – touching a keyboard, touching certain fabrics (rare), being touched by another person
Other Triggers – vibration from anything such as bass, bumping desk, kicking chair, heavy footsteps
Here are some rates of occurrence of visual triggers from my 2015 survey.
| Open mouth chewing | 78% |
| Leg jiggling, foot wiggling | 48% |
| Jaw movement | 42% |
| Repetitive hand movement such as twiddling thumbs, touching face, biting nails, picking at cuticles, etc. | 39% |
| Single hand movement such as touching face, pointing, or moving food to mouth | 24% |
| Hair twirling, hair touching | 17% |
| Other | 9% |
I want to point out that the average misophonia severity reported in my 2015 survey for the above triggers was 14 on the A-Miso-S (which is the top of the moderate severity rating) and 40 on the Misophonia Assessment Questionnaire (which is the lower end of severe severity rating). Most of those responding to the survey (90%) had at least one visual trigger.
Dog drinking is frequently reported as a trigger. One reason for this is that dog’s drink with the bottom of their tongue. They actually curl the tip of their tongue under to make a scoop and throw the water into their mouth. It is messy and loud, but very efficient. It is better to think dogs as efficient drinkers rather than messy and loud drinkers. Loud is bad, but efficient is good.
4. Oh, the Emotions!
An extreme emotional response is the trademark of misophonia. Here is a comment someone with misophonia posted on misophoniatreatment.com.
“I have only recently found out that there was a name for my condition. I am fifty-four years old have suffered what seems like forever with this problem. One particular person at work drives me crazy sniffing and coughing all the time. At times I get so I angry I think I could kill. I even get to the point of wishing this person would drop dead (bad I know), but I’m sure other sufferers feel the same at times. My poor lovely husband knows how I feel and tries his best not to make the noises I detest. I sometimes don’t know how he lives with me. I know I have passed this on to one of my girls, and my dad had it, too. It’s making my social life a nightmare.”Note that she wishes the person making the noise would drop dead! It is hard for someone who does not have misophonia to understand the extent of emotions that are caused by being repeatedly triggered, especially in a situation where the misophonic individual is trapped and cannot make the triggers stop.
Misophonia in the News
On April 16, 2015, Southwest Airlines flight 577 was taxiing toward the runway at Chicago’s Midway International Airport en route to Manchester, New Hampshire. An elderly, white haired man, Lenny Mordarski, went to sleep and started snoring. The woman sitting beside him stabbed him repeatedly in the arm with her pen to stop him from snoring. Lenny said it felt like he was being stung by bees. The airplane returned to the gate and shortly thereafter took off for Manchester, without the assailant. Thanks to Lenny’s long sleeve shirt, no blood was drawn. The woman in question was placed on a later flight.Feeling trapped with triggers makes the emotional responses worse. The poor woman likely felt trapped but tried to ignore the snoring until she could bear it no longer. It probably didn’t take long for her to reach this point. Her fight-or-flight response took over, and she attacked.
Below is a twenty-six-question survey of emotional responses to triggers. I use this survey for my new misophonia clients. As you read through these, you will see that the list of emotions/reactions go from mild to extreme. All of these emotions are often rated as “none of the time,” “a little of the time,” “a good deal of the time,” or “almost all the time.”
Misophonia Emotional Responses
0) None of the time, 1) A little of the time, 2) A good deal of the time, 3) Almost all of the time
- You hear a known trigger sound. You may dislike the sound.
- You hear a trigger sound and feel annoyed or upset.
- You want the other person to know how upset you are.
- You want the person to stop making the sound.
- You want to force the other person to stop making the sound.
- You feel you must see that the person is actually making the sound or doing what you think they are doing. You want to keep looking or stare.
- You want to hear something else, so you don’t hear the sound.
- You want to be physically far away from the sound.
- You wish you were deaf.
- You are afraid that if you do something you will hurt others’ feelings.
- You want to get away from the sound but do not want to make a scene.
- You want to get away from the sound as quickly as possible, even if it would be embarrassing.
- You want to push, poke, shove, etc., the person making the sound.
- You want to verbally assault of the person making the noise.
- You want to physically assault the person making the noise.
- You want to physically hurt or harm the other person.
- You want to scream or cry loudly.
- You feel anger.
- You feel rage.
- You hate the person.
- You feel disgust.
- You feel resentment.
- You feel you need to escape, flee, or run away.
- You want to get revenge.
- You feel offended by the person making the noise.
- You feel despair or hopeless.
- You feel guilt while you are being triggered.
- You feel guilt after you calm down from being triggered.
- You feel fear of more triggers to follow.
- You feel fear (immediate, at that moment)
One person may respond with “not at all” to a few of these questions, but most people with misophonia experience over 75% of the feelings expressed on this list. In general, individuals will have all of these emotions (rated 1, 2, or 3) except for two or three, which are unique to each individual. Misophonia causes extreme emotions in virtually everyone.
In our recent study on the initial physical and emotional responses to triggers, we exposed individuals to a tiny, super weak trigger and asked them to report their physical sensation and emotions. The triggers were short and quiet, and only one at a time. The emotional responses were generally mild, such as irritation, mild disgust, annoyance, mild fear, etc., because the triggers were very weak. The table below shows the emotions reported by the 26 participants who were tested for two auditory triggers and one visual trigger. The categories of emotion are aggregations of similar emotions. For example, aggravation, irritation, annoyance, frustration, anger, and rage are combined into the anger category. All individuals (100%) reported an emotional response to at least one of their tested triggers.
| Emotional Response | Number of Participants
(n=26) |
% of Participants |
| Anger | 24 | 92.3% |
| Anxiety | 24 | 92.3% |
| Desire for Escape | 14 | 53.8% |
| Disgust | 12 | 46.2% |
| Fear | 6 | 23.1% |
| Sadness | 4 | 15.4% |
| Other | 9 | 34.6% |
| None | 8 | 30.8% |
The triggers for these tests were very mild, such as one bite into a small piece of lettuce. But the triggers still (usually) produced an immediate, negative emotion. How can this be? How can a short, soft sound cause an immediate emotion?
Sukhbinder Kumar, Ph.D. explained his research on this topic in his presentation at the 2015 Misophonia Association Conference in Chicago and in the journal article, The Brain Basis for Misophonia.[xi] Dr. Kumar observed the brains on individuals exposed to trigger sounds with fMRI (functional magnetic resonance imaging). fMRI shows brain activity by measuring blood flow. Where more blood is flowing, there is more neuronal activity. The study compared 22 people with misophonia vs. 20 without misophonia. In response to trigger sounds, the people with misophonia had higher activity in the anterior insula, which is known to be involved in sensing inside the body and external senses (hearing, sight, taste, touch, and smell) and internal sensations (pain, stomach ache, muscle tension, etc.). Other research indicates that the anterior insula is involved in subjective feelings of emotions.
No surprise here. We would all expect to see greater emotional brain activity for an individual with misophonia. The study also showed a connection between activity in the anterior insula and the vmPFC (ventromedial prefrontal cortex) and posteromedial cortex (PMC). These structures are key parts of is called the Default Mode Network which is involved in retrieval of memory. (For simplicity, I will only mention the vmPFC to indicate both the vmPFC and PMC.) This connectivity is very important because the vmPFC and is known to be involved in associative learning (or learning from experience). Essentially, this research shows that the brain response to trigger stimuli is a conditioned (learned) emotional response (an involuntary emotional reflex response). An individual with misophonia hears/sees a trigger and “boom” there is an instant, involuntary emotion forced on the person. With misophonia, the person does not choose how to feel after a trigger, it just happens automatically.
For individuals without misophonia, the vmPFC acted to reduce activity in the anterior insula. Additionally, for individuals with misophonia, there was high activity between the anterior insula and the hippocampus and between the anterior insula and the amygdala.
The following figure is from Dr. Kumar’s journal article. It illustrates the increased connectivity between these regions of the brain when person with misophonia is exposed to a trigger stimulus. It is used with permission from the journal article
Kumar et al., The Brain Basis for Misophonia, Current Biology (2016), http://dx.doi.org/10.1016/j.cub.2016.12.048
In the figure that follows,
- The anterior insula is the center image
- The vmPFC is the upper right image
- The PMC is the upper left image
 I exchanged email to clarify Dr. Kumar’s view of this and he provided the following quotes. “In misophonic subjects… the connectivity between vmPFC and anterior insula is positive, indicating that vmPFC, rather than regulating, is boosting the activity of anterior insula.” And, “Given the role of vmPFC in learning associations, our data is consistent with the view that aberrant associations represented in vmPFC drive areas involved in emotion processing.”
I exchanged email to clarify Dr. Kumar’s view of this and he provided the following quotes. “In misophonic subjects… the connectivity between vmPFC and anterior insula is positive, indicating that vmPFC, rather than regulating, is boosting the activity of anterior insula.” And, “Given the role of vmPFC in learning associations, our data is consistent with the view that aberrant associations represented in vmPFC drive areas involved in emotion processing.”
Here is my interpretation in plain English.
- In individuals with misophonia, the vmPFC is supercharging the emotional response to the triggers, but in the controls the vmPFC is dampening the response.
- Misophonia emotions are an acquired emotional reflex (a conditioned emotional response or CER)
- The emotional response develops through experience with triggers.
- The emotions are an involuntary reflex response.
- The emotions from a trigger are not a choice of the person. Rather, they are activated or instantly inserted into the brain.
5. Oh, the Guilt!
Generally those suffering with misophonia feel guilty about the way they think and act when being triggered. We typically reserve the list of powerful emotions discussed in the previous chapter for our worst enemies or times when we’re greatly offended, but people with misophonia regularly direct these responses to those who are closest to them. The ugly miso-emotions are literally jerked out of the misophonic individual when they are being triggered. Additionally, once the fight-or-flight response kicks in, the person may scream, verbally assault, or even push, poke, and shove the person who caused the trigger. If looks could kill, everyone around the misophonic person would be dead!
Nearly everyone with misophonia feels a varying degree of guilt after being triggered. Most feel a great deal of guilt because they recognize that their response was out of proportion to what the triggering person did. For example, children are often triggered by a parent, which causes these extreme negative emotions to be directed at their primary attachment figure. One person reported that their trigger person was his stepfather, whom he dearly loved. He was a great man, even his hero. But when riding in the car, the stepdad would chew gum, and suddenly the child experienced nearly every emotion affiliated with misophonia, including wanting to hurt his stepdad. Afterwards, the person felt guilty for wanting to hurt someone, especially someone he loved so dearly.
Guilt is also very common for a parent who has a child that triggers them. The love of the parent for the child is inconsistent with the rage felt toward that child for making an innocuous sound like sniffling. Again, guilt follows.
Misophonia generally develops to sounds made by someone who spends a lot of time with the misophonic individual. Except in cases where there is an embroiled relationship that is full of conflict, abuse, and contention, the strong miso-emotions are directed toward a loved one, and are inconsistent with the emotional bond with that person. Guilt is common when we act differently than we think we should act, which is why it is such a recurring emotion among individuals with misophonia.
If you have misophonia, have compassion for yourself. Guilt is the feeling a person has when they have intentionally done something wrong. If a child steals candy from the store, then they should feel guilty for doing that. If a sales clerk accidentally gives you five dollars extra in change and you know it, you should feel guilty for keeping the money because you chose to do something that was not honest. But if you get the extra change, only to discover it later, you should not feel guilty because you did not do choose to do something that violates your moral values.
If you have misophonia, you may have horrible feelings toward a loved one; but you are not choosing to have these feelings. These feelings are literally yanked out of you, or imposed on you by your misophonia. They are not really “your” feelings or feelings you have decided to express toward that person. They are an emotional reflex. As previously discussed, a reflex is an involuntary response to a stimulus. In this case, the emotions simply happen as a direct result of being triggered.
Because you are not choosing to have horrible feelings toward a person you love, try replacing your guilt with regret. You don’t want to have such ill feelings about someone after they trigger you, and you regret that you have them. If you want to be tall, but your height is only five feet, then you can regret that you are not taller; but because it is not your choice, guilt would be an inappropriate emotion. So be good to yourself. Beating yourself up and feeling guilty about your miso-emotions doesn’t help in any way. Anything that decreases your feeling of well-being will increase your misophonia. So smile, and realize that at this stage, the extreme miso-emotions are beyond your control.
However, there is hope! You do have a degree of control over how you respond when you have misophonia triggers. These are your coping behaviors. If your coping behaviors (fifth box on the drawing below) are aggressive, then you can and should work to change those. But this change is not easy, and it takes time and concerted effort.
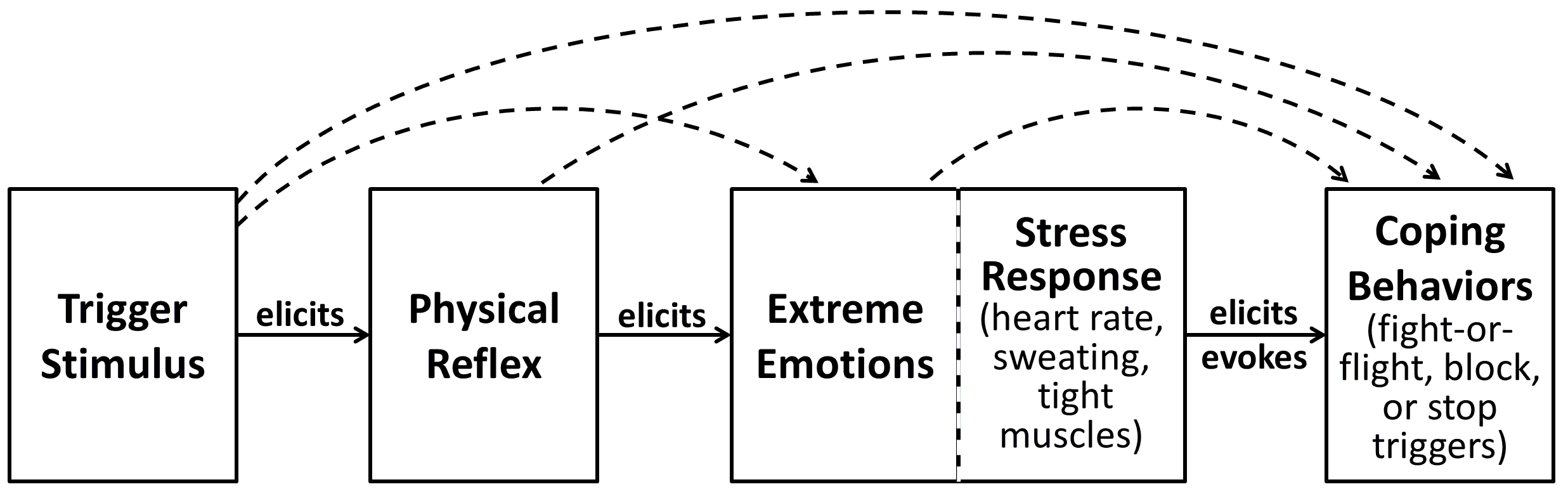
Although difficult, you can (and should) work to manage your coping behaviors by deciding what you want to do when you are triggered. The change may be slow, but keep trying. A good therapist can help you with this. One of the easiest ways of reducing aggressive coping behaviors is to reduce the number of triggers you experience, especially situations where you cannot escape the triggers. I know it sounds like a lot for now, but relax: we will talk more about how to do this in the chapter on misophonia management techniques. For now, I just want you to stop beating yourself up over the things you’ve felt and said as a result of your misophonia, and instead take the time to regret some of your misophonia-induced feelings and behaviors.
6. Prevalence of Misophonia
How common is misophonia? Many consider it a rare disease, and on rare disease day (the last day of February), many on the Facebook misophonia group express a desire to speak out about misophonia. In the United States, a rare disease has officially been defined as one that affects less than 200,000 people in the US, which is about one in 1,500 people (0.07%). By this definition misophonia is not a rare disease. It is a “rarely known” disorder.
I did my first survey on misophonia in February of 2013 on different characteristics of individuals with misophonia. I was trying to determine how misophonia develops and if there were certain characteristics people with misophonia have in common. I wanted to have a control group to compare some of the personality traits and characteristics, and so I sent the survey to my LinkedIn contacts. Much to my surprise, 5% of my LinkedIn contacts had misophonic reactions. And so I thought, wow, this is not some extremely unusual phenomenon here. In fact, I had people with misophonia popping up all over the place.
I paid for a survey using SurveyMonkey.com, where they randomly solicited individuals who had no connection to misophonia. These were just individuals who were willing to fill out surveys to have fifty cents donated to the cause of their choice. I purchased three hundred and I got ten extra for free. I made sure that the title of the survey did not mention sound or sensitivities. I gave the same survey to a group of people with misophonia to determine a standard of reference for my Survey Monkey group. Out of the 310 people surveyed (50% of them women, 50% men), I found that 15.2% had reactions suggesting misophonia. It was more common among the women (18.6%) than it was among of the men (11.6%).[xii] Rather than being a rare disease, which is one in 1,500, it was a rarely known but common disorder with about 225 in 1,500 having misophonia.
That was actually a higher number that I expected. I was expecting 5% to 10%, but it came in at 15%. In 2014, there was a published peer-reviewed study that came out of the University of South Florida’s College of Medicine and their psychology department. They used undergraduate psychology students. (This is very common in college research; they give psychology students a little extra credit for taking a survey or participating in some form of research for the graduate students.) They had almost 500 participants in this study, and 84% were women. Their study was comprehensive enough to see how the misophonia affected the individual’s life. They found that 20% had clinically significant misophonia,[xiii] significant meaning they had to spend a good deal of conscious energy resisting or being affected by triggers. They did not find any statistical difference in the prevalence of misophonia in men vs. women.
A recent blog post on the family ancestry website 23andMe.com mentioned an internal study conducted with about 80,000 customers, in which people were asked “Does the sound of other people chewing fill you with rage? (Yes/No/Not Sure).” About 19% replied yes. They also found that the affirmative response was more common in women.[xiv] 23andMe reported 20% yes and 80% no (excluding the not sure responses). One internet post indicated there were about 4% not sure. So that would reduce the percentage of “yes” responses from 20% to 19%.
A 2015 PhD dissertation on decreased sound tolerance (hyperacusis, tinnitus, and misophonia) reported 15.6% of participants with clinically significant misophonia, in a mix of college students and community participants[xv]. A higher percentage of males reported misophonia symptoms, but females reported greater severity. This provides further support for the surprisingly high prevalence of misophonia.
The takeaway from this is that misophonia is really quite common – perhaps affecting approximately 15% of adults (or 1 in 6.5 adults). It seems to be more common (or at least more severe) in women than in men, but many, many people suffer in silence, or they are written off as being grouchy, cranky, or irritable. If this number is correct, and research is beginning to confirm it is, there could be forty million people with misophonia in the United States alone – that is 40,000,000 people.
Considering these statistics and the fact that misophonia is not widely studied, if you randomly selected a doctor or therapist and then another individual, it is more likely that the random individual would have misophonia than the doctor or therapist would know about misophonia.
[i] Jastreboff & Jastreboff, 2002
[ii] Bernstein, Angell, & Dehle, 2013
[iii] Bernstein, Angell, & Dehle, 2013; Dozier, 2015a; Johnson et al., 2013; Schröder, Vulink, & Denys, 2013
[iv] Schröder, Vulink, & Denys, 2013
[v] Schröder, Vulink, & Denys, 2013
[vi] Dozier, Lopez, & Pearson, in review
[vii] Wu, Lewin, Murphy, & Storch, 2014; Cash 2015
[viii] Schröder, Vulink, & Denys, 2013. Note: This form has been modified by replacing “sounds” with “triggers” to include visual and sound triggers.
[ix] Johnson, 2014
[x] Wu, Lewin, Murphy, & Storch, 2014; Cash 2015
[xi] Kumar, 2015
[xii] Dozier, 2014
[xiii] Wu, Lewin, Murphy, & Storch, 2014
[xiv] Accessed from http://blog.23andme.com/23andme-research/something-to-chew-on/ on June 7,2015
[xv] Cash, 2015